





Interventional radiologists are central to creating, troubleshooting, and prolonging the life of haemodialysis access using minimally invasive, image-guided techniques. They function as procedural experts within a multidisciplinary vascular access team alongside nephrologists and surgeons to keep patients on effective dialysis with minimal catheter dependence.
Core clinical roles
- Access creation and bridging
Interventional radiologists place tunneled and non-tunneled dialysis catheters when urgent haemodialysis is needed or while waiting for AV fistula or graft maturation. In selected centers, they also perform image-guided or endovascular AV fistula creation, expanding options in patients with challenging anatomy - Diagnosis of access dysfunction
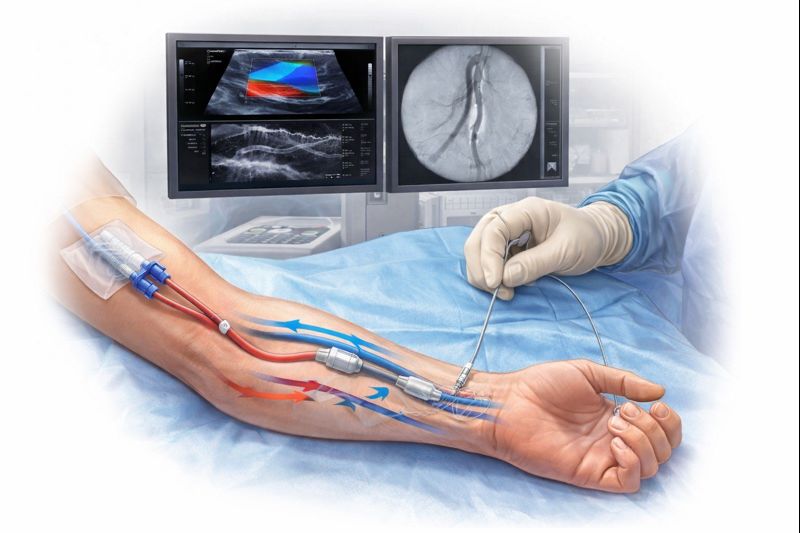
They perform and interpret duplex ultrasound and fistulography to map the entire access circuit, identify stenosis, thrombosis, pseudoaneurysms, and central venous disease. These studies guide targeted therapy and help differentiate lesions that need simple angioplasty from those requiring stents, complex recanalization, or surgical revision
Endovascular maintenance and salvage
- Angioplasty, stents, and stent-grafts
Interventional radiologists perform percutaneous transluminal angioplasty to treat inflow, outflow, and central venous stenoses, restoring access flow and dialysis adequacy. Where there is recoil, recurrent stenosis, or rupture risk, they deploy bare-metal stents or covered stent-grafts to scaffold and seal the vein - Declot and thrombosis management
For acutely thrombosed AV fistulas and grafts, they perform pharmacologic thrombolysis combined with mechanical thrombectomy to rapidly re-establish patency and avoid new catheter placement. Treating the culprit stenosis in the same sitting reduces early rethrombosis and improves cumulative access survival
Central venous and catheter-related work
- Central venous stenosis and occlusion
Interventional radiologists diagnose and treat catheter- or device-related central venous stenosis/occlusions with angioplasty, stenting, and advanced recanalization techniques, often enabling continued use of a threatened access. In complex “end-stage” access situations, they support placement of specialized devices such as HeRO grafts through endovascular maneuvers that many surgeons do not routinely perform - Catheter management
They handle image-guided catheter insertions, exchanges, repositioning, and removals, and manage fibrin-sheath–related dysfunction with sheath disruption or angioplasty. By efficiently rescuing failing catheters yet prioritizing transition to permanent access, they help reduce infection, thrombosis, and central venous injury
Multidisciplinary and longitudinal care
- Part of a dedicated access team
Modern haemodialysis programs rely on teams that include nephrologists, vascular or transplant surgeons, and interventional radiologists to coordinate referral timing, imaging, interventions, and follow-up. Such teams are associated with higher fistula use, fewer catheters, and better overall access outcomes - Protocol development and quality improvement
Interventional radiologists contribute to local algorithms for surveillance triggers, pre-emptive intervention thresholds, and post-procedure care, aligning with contemporary vascular access guidelines. They also drive adoption of new devices and techniques for access creation and maintenance, improving durability and patient experience over time